Dental Crowns

Dental crowns are the gold-standard restoration for damaged, weakened, or cosmetically compromised teeth combining protection with natural aesthetics. As one of the most common dental procedures, a crown dental restoration at Vitrin Clinic delivers results that look and feel entirely natural.
Treatment Process
A clear step-by-step overview of how the treatment is planned and performed, from the initial consultation to the final results, ensuring comfort, safety, and predictable outcomes.
01
In-Depth Consultation & Imaging
Comprehensive examination of your oral health, bite alignment, and treatment goals. 3D scans and digital bite-mapping for precision planning tailored to your specific case.
02
Tooth Preparation
Gentle removal of decayed or damaged enamel. The tooth is sculpted into a form that supports a perfect crown fit. Highly accurate digital or physical impressions are taken.
03
Fabrication
A temporary crown is placed for crowns made externally in the lab. For same-day cases, CEREC precision milling is performed on-site for instant turnaround.
04
Fitting & Bonding
Trial fit to assess form, colour, and function. Final bonding with ultra-strong adhesive. Bite adjustment ensures comfort and correct alignment.
05
Finishing, Polish & Aftercare
Polished to replicate natural tooth sheen. Final check on contact points and aesthetics. Post-placement guidance on hygiene and follow-up scheduling included.
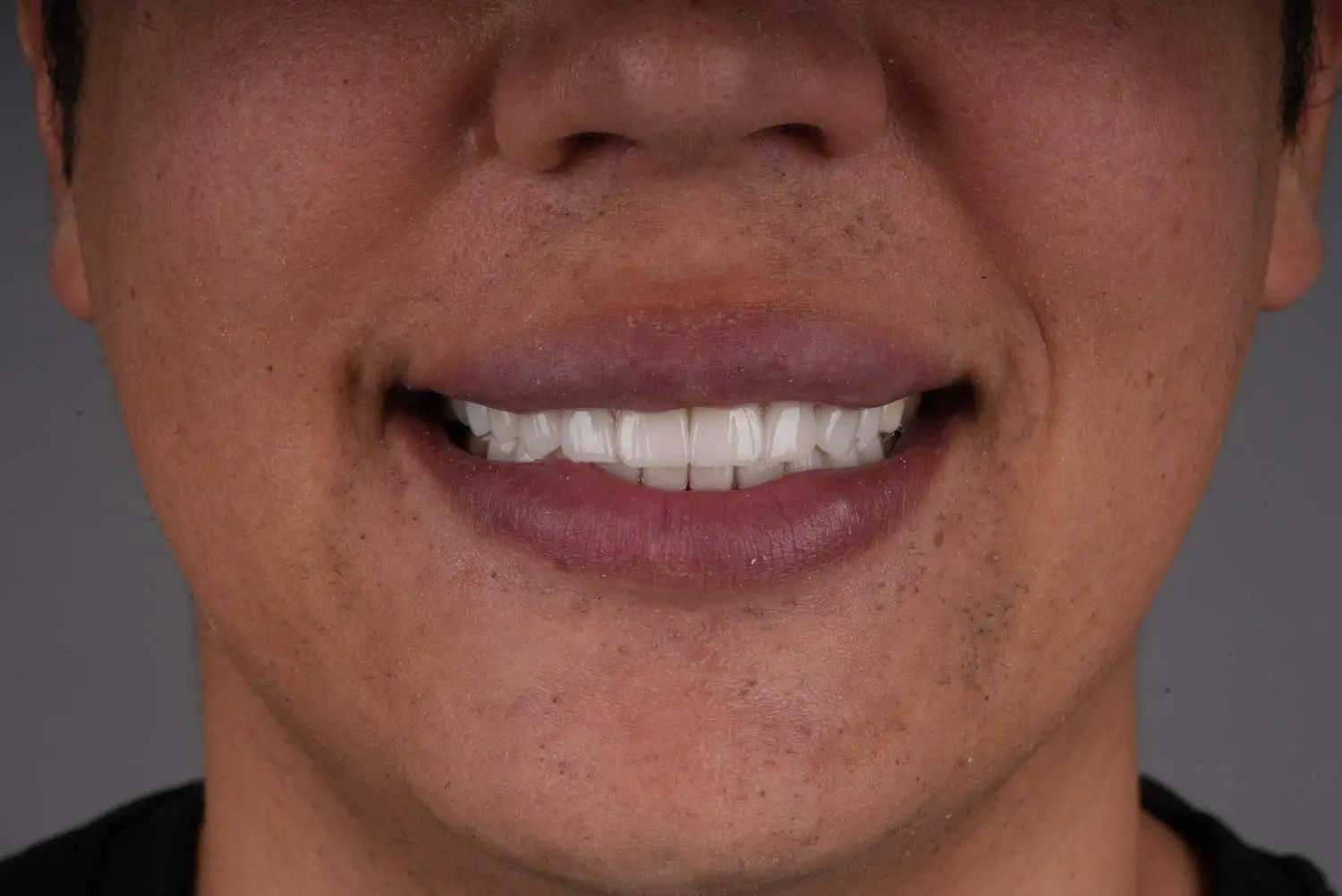
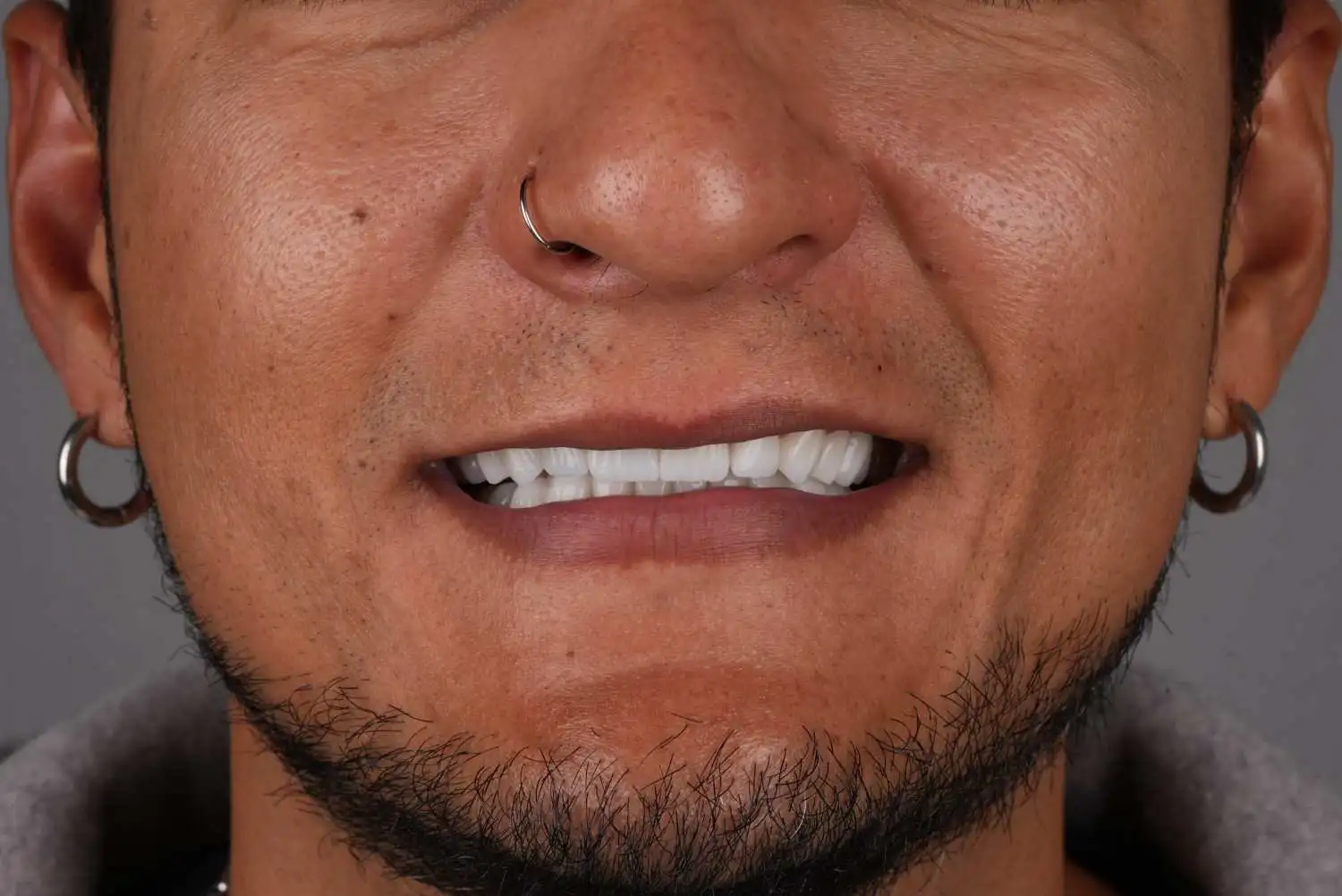
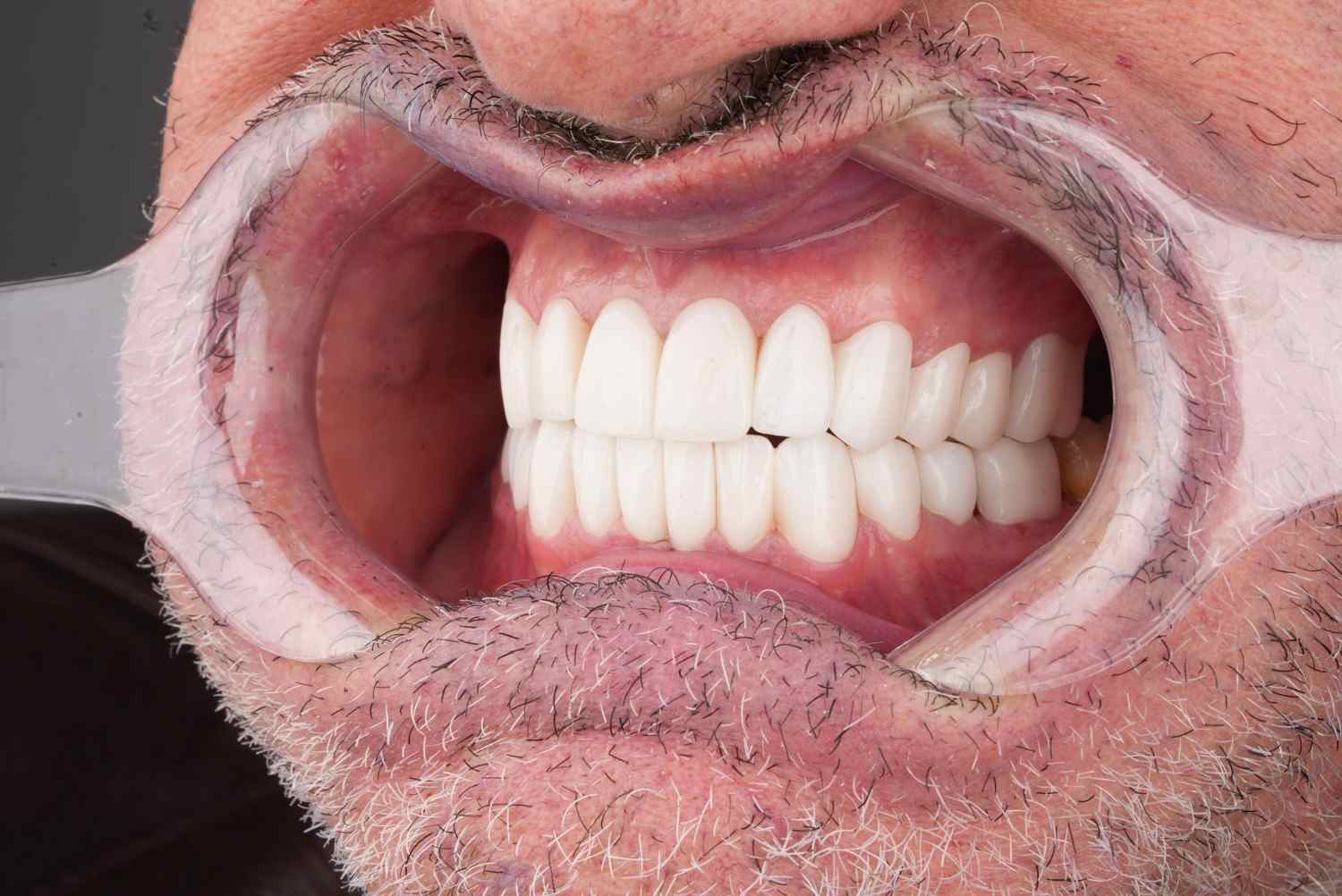
Before & After Results
Real patient transformations showcasing the quality, precision, and care behind our dental treatments. Results are personalized to each patient's needs and goals.







.webp)

What Is a Dental Crown?
A dental crown is a full-coverage restoration that encases the entire visible portion of a tooth above the gum line restoring its shape, size, strength, and appearance to full clinical function.
Unlike a veneer, which covers only the front surface of a tooth, a crown envelops the tooth on all sides, providing structural reinforcement where the underlying tooth structure is insufficient to support a partial restoration alone.
The clinical decision to place a crown rather than a veneer, onlay, or direct composite restoration is determined by the extent of remaining tooth structure, the functional demands on the tooth, and the aesthetic requirements of the individual case.
At Vitrin Clinic, crown placement is recommended only where the clinical evidence supports it as the most appropriate and durable solution for the patient's specific tooth condition.
98.5%5-Year Survival Rate | 15–20+Years Longevity | 2Visits to Complet | 360°Full Tooth Coverage |
|---|---|---|---|
When Is a Crown Clinically Indicated?
The decision to crown a tooth is a clinical judgement, not a cosmetic preference.
Crowns are the restoration of choice in specific clinical situations where partial coverage restorations veneers, onlays, or direct composites cannot provide sufficient structural protection or predictable long-term outcomes.
Understanding the indications is essential to ensuring the right restoration is placed for the right reasons.
Extensively Damaged or Decayed Teeth
Where dental caries or fracture has destroyed a substantial portion of a tooth's coronal structure, a crown is the only restoration capable of replacing the lost volume while protecting the remaining tooth from further fracture.
Direct composite restorations become progressively less reliable as cavity size increases full coverage provides structural integrity that partial restorations cannot replicate once a critical threshold of tooth structure is lost.
Endodontically Treated Teeth
Teeth that have undergone root canal treatment lose structural integrity the pulp chamber, which contributes to tooth hydration and resilience, is removed, and the access cavity preparation further reduces coronal structure.
Systematic review evidence confirms a long-term survival advantage for crowning endodontically treated posterior teeth over composite restoration alone.
The ferrule effect a circumferential band of sound dentin 1.5 to 2 mm above the preparation margin is clinically established as the single most important structural factor determining crown longevity in root-treated teeth.
Cracked or Fractured Teeth
Teeth with confirmed or suspected cracks characterised by pain on biting, temperature sensitivity, or visible crack lines require full cuspal coverage to prevent crack propagation to the root.
A veneer or onlay does not provide circumferential protection.
A crown binds the tooth from all sides, stabilising existing cracks and preventing the forces of occlusion from driving them apically into the root, where the result would be extraction.
Severely Worn Teeth
Tooth surface loss from bruxism, acid erosion, or attrition can reduce teeth to a fraction of their original height, compromising aesthetics, bite, and the ability to chew effectively.
Where wear is extensive enough that veneers cannot restore the correct length without significant preparation into dentine, full-coverage crowns provide the volume of material needed to re-establish tooth height and occlusal function without compromising the underlying tooth further.
Crown on a Dental Implant
Implant-supported crowns are the final restorative component of a dental implant the ceramic crown attached to the abutment that connects to the titanium implant post.
Once the implant has fully osseointegrated, a custom ceramic crown is fabricated to match the surrounding natural teeth in shape, colour, and bite position.
Crowns vs. Veneers vs. Onlays vs. Direct Restoration
The appropriate restoration depends on how much tooth structure remains, what the tooth has to endure functionally, and what the aesthetic goals are.
This comparison is drawn from peer-reviewed clinical outcome data and evidence-based restorative guidelines.
Criterion | Full Crown | Porcelain Veneer | Onlay / Partial Crown | Direct Composite |
|---|---|---|---|---|
Tooth Structure Preserved | Least conservative , full circumferential reduction | High, facial surface only | Moderate - cuspal coverage only | Highest - additive or minimal prep |
Indicated for Structural Damage | Yes, primary indication for extensive damage | No, requires intact tooth structure | Moderate - suited to partial damage | Small cavities only |
Endodontically Treated Teeth | Gold standard - especially posterior teeth | Not indicated | Suitable for some presentations | Not recommended for posterior ETT |
Crack Protection | Full , binds tooth from all sides | No circumferential protection | Partial - depends on coverage design | No fracture protection |
5-Year Survival Rate | Up to 98.5%- monolithic lithium disilicate | 95.5% - PLV meta-analysis (6,500 restorations) | 95–99% short-term, variable long-term | Variable - 5–10 years average |
Aesthetics | Excellent, full control of shape, shade, contour | Excellent - natural enamel-like translucency | Good - partially visible margins | Good initially - stains over time |
Reversibility | Irreversible, extensive preparation | Partially irreversible -enamel reduction | Partially irreversible | Reversible - no tooth structure removed |
Bruxism / High Occlusal Loading | Zirconia crowns suited to parafunctional cases | High fracture risk in bruxism | Depends on material and coverage | High wear and fracture risk |
Compiled from: PubMed — Survival Rates of Metal-Ceramic, Veneered and Monolithic All-Ceramic Single Crowns (64 studies, 11,560 crowns, 2026) · Malmö University / Qassim University — Long-Term Survival of PLVs, PMC7961608 · NIH/PMC — Remaining Tooth Structure and Prognosis of Endodontically Treated Teeth, PMC12604680 · King Saud University — Clinical Outcome of Full-Coverage Crown vs. Indirect Bonded Restoration on ETT, PMC11501469.
What the research shows
98.5% | 1.5–2mm | 99% |
|---|---|---|
5-year survival rate for monolithic lithium disilicate crowns the highest recorded across all crown materials in the most comprehensive meta-analysis to date, evaluating 11,560 crowns across 64 studies with minimum 3-year follow-up | The clinically established minimum ferrule height for endodontically treated teeth — the circumferential band of sound dentin above the preparation margin that is the single most important structural determinant of crown longevity in root-treated teeth. | 10-year survival rate for endocrown restorations on endodontically treated posterior teeth a monolithic full-coverage alternative that eliminates the need for a post-and-core and maximises remaining tooth structure, reported in peer-reviewed NIH/PMC literature. |
PubMed Survival Rates of Metal-Ceramic, Veneered and Monolithic All-Ceramic Single Crowns, 2026 · PMID 41489982 | NIH/PMC Remaining Tooth Structure and Prognosis of Endodontically Treated Teeth, PMC12604680 · PubMed Ferrule Effect: A Literature Review, PMID 22152612 | NIH/PMC Endocrown Adaptation and Retentive Strength: Clinical Evidence, PMC10828905 |
Vitrin Clinic Standard
You will be told why a crown is the right choice for your tooth
The clinical indication for your crown is explained clearly before any preparation begins. If a more conservative restoration is appropriate, we will recommend it instead.
Material selected for your specific tooth, not by default
Lithium disilicate, zirconia, or another material is chosen based on where the tooth sits, how hard you bite, and what aesthetic result is needed — not a blanket policy.
Provisional crown on the day no unprotected preparations
You leave your preparation appointment with a provisional crown in place, shaped to the planned design, so your tooth is protected and your appearance is maintained during the laboratory period.
Final crown verified before cementation not after
Fit, margin accuracy, shade, and bite are all confirmed during the try-in phase. If anything requires adjustment, it goes back to the laboratory. We do not cement and correct.
Dental Crown Cost: vitrin Clinic vs. UK vs. USA
The cost of a dental crown varies depending on the material selected, the clinical complexity of the case, and the country of treatment.
The following table provides a transparent comparison of average costs by crown type across the United Kingdom, United States, and Vitrin Clinic in Istanbul allowing patients to assess their options accurately before their consultation.
Crown type | 🇬🇧 UK | 🇺🇸 USA | 🇹🇷 Turkey |
|---|---|---|---|
Zirconia crown Monolithic, high strength per unit | $890 – $1,525 | $1,000 – $2,500 | From $150 / unit |
E.max crown Lithium disilicate, premium aesthetics per unit | $1,270 – $2,030 | $1,200 – $2,500 | From $180 / unit |
PFM crown Porcelain-fused-to-metal per unit | $570 – $1,015 | $800 – $1,500 | From $100 / unit |
CEREC same-day crown CAD/CAM milled, single visit per unit | $1,015 – $1,780 | $1,000 – $2,000 | From $200 / unit |
Consultation & scans | Charged separately | Charged separately | Free & included |
Estimated saving | — | — | Up to 70% less |
* Prices are averages for reference only and may vary based on individual case requirements, tooth location, material selection, and treatment complexity. A personalised quote is provided following your free consultation.
Clinical Evidence & References
University of Bern, Switzerland Landmark Systematic Review
All-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses Systematic Review, Part I: Single Crowns
Clinical Oral Implants Research · 2015Pjetursson BE et al. · PubMed PMID: 25842099 · 67 studies, 13,097 crowns
Key finding: 5-year survival of metal-ceramic crowns 94.7%. Lithium disilicate and leucite-reinforced glass ceramic crowns achieved comparable 5-year survival rates of 96.6%, confirming all-ceramic systems as a clinically equivalent alternative to metal-ceramic for single crown restorations.
King Saud University, Riyadh, Saudi Arabia
Clinical Outcome of Indirect Bonded Porcelain Restoration Versus Full-Coverage Crown on Endodontically Treated Teeth in Posterior Areas Systematic Review
Cureus · September 2024Alhamdan MM, Alghuwainem N et al. · DOI: 10.7759/cureus.70116 · PMC11501469
Key finding: Full-coverage crowns demonstrate superior long-term survival for endodontically treated posterior teeth with extensive structural loss. Partial indirect restorations are a valid alternative for teeth with sufficient remaining cuspal structure but are not equivalent for significantly compromised posterior teeth.
Rungta College of Dental Sciences and Research, India
Effect of Ferrule Height on the Fracture Resistance of Endodontically Treated Teeth Restored with Glass Fiber Posts
Cureus · February 2025Rathaur S, Gupta PK et al. · DOI: 10.7759/cureus.79583 · PMC11946697
Key finding: Fracture resistance increases significantly with ferrule height in endodontically treated teeth restored with fiber posts and full crowns. A 2 to 3 mm ferrule produces measurably higher fracture loads and more favourable failure patterns than restorations without ferrule reinforcing ferrule assessment as a non-negotiable step before crown preparation of root-treated teeth.
Frequently Asked Questions
Answers to common questions about the treatment, including suitability, procedure details, recovery, and long-term care — helping you feel informed and confident before moving forward.











