Dental Implant
September 10, 2025
What is a Bone Graft and Why Choose Turkey in 2026?

Bone graft procedures are often the first step toward successful dental implants if you've experienced jawbone loss. If you're planning to get dental implants but have been advised to undergo a bone graft, don't worry, you're not alone. Many patients need jaw bone augmentation to restore lost or weakened bone and support successful tooth replacement. At Vitrin Clinic, we specialize in procedures that rebuild the jaw using advanced techniques and materials, including bone marrow or synthetic grafts. In this guide, we'll cover the essentials: why this treatment is needed, the different types, healing stages, costs, and how our expert team ensures safe, effective results.
What Is a Bone Graft for Dental Implants?
A dental bone graft is a surgical procedure that rebuilds the jawbone which has thinned, shrunk, or lost density. This most often happens after tooth loss, gum disease, or trauma. It's needed before a dental implant because implants depend on solid bone to fuse with and stay stable for years. Without enough bone volume, an implant can shift, loosen, or fail to integrate properly. At Vitrin Clinic, detailed imaging determines exactly how much bone rebuilding your case requires before any surgery is ever planned.
The Purpose of Bone Grafting Before Dental Implants
This procedure adds bone to your jaw where it has deteriorated or lacks density. When tooth loss occurs, whether from trauma, decay, or gum disease, the surrounding bone begins to shrink within months. This bone loss can prevent dental implants from anchoring securely. Implants need a firm, thick foundation to fuse with over time. This treatment restores that foundation. It gives implants the strength and long-term stability needed for a lasting, functional result.
When Do You Need a Bone Graft for an Implant?
You may need this procedure for a tooth implant if:
Your jawbone is too soft or thin to support an implant
You've had missing teeth for a long time
You've experienced bone loss due to infection or injury
At Vitrin Clinic, our expert team uses advanced imaging to determine exactly how much grafting you need. We also offer free consultations to help you plan with confidence. Learn about the Cost of dentures in Turkey and how affordable options can restore your smile. Also discover how Full‑mouth dental implants cost in Turkey can provide a complete smile makeover for patients with several missing teeth and significant bone loss.
The Bone Graft Procedure: Step-by-Step Process
The bone graft procedure follows four clear stages: an initial consultation with 3D imaging, selection of the right graft material, the surgical placement itself, and a healing period where the graft fuses with your natural bone. Each stage is planned carefully to keep the process safe and comfortable. At Vitrin Clinic, patients are guided through every step, from the first scan to full integration, with no surprises along the way.
Initial Consultation and Imaging
Your journey starts with a 3D scan or X-ray to assess your bone density. This also maps the exact shape of your jaw. At Vitrin Clinic, this initial exam is part of your complimentary consultation, so there's no cost or pressure. This imaging step lets our implantologists identify weak spots and measure available bone. From there, they design a grafting plan tailored precisely to your anatomy and treatment goals.
Types of Bone Graft Materials Used
Different graft materials may be used depending on your case. All of them are safe, biocompatible, and proven to integrate with human bone over time. These include your own bone, donor bone, animal-derived bone, and synthetic minerals. Each offers a different balance of strength, safety, and convenience. Your Vitrin Clinic implantologist selects the material that best matches your bone quality, the size of the defect, and your personal treatment preferences.
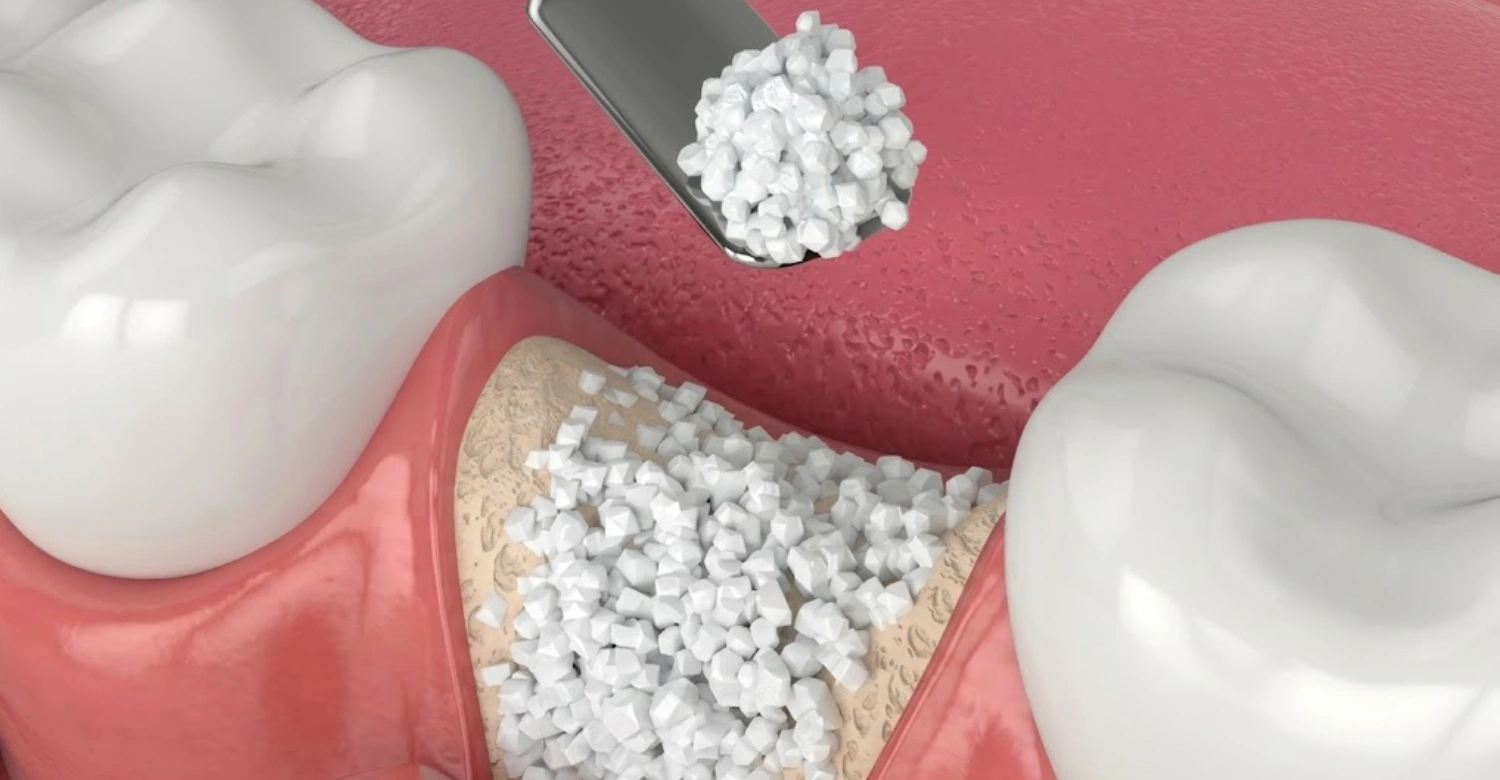
Surgical Procedure Explained
The dentist numbs the area, makes a small incision, and places the bone material where it's needed to rebuild lost volume. Sutures are applied, and healing begins almost immediately afterward. The procedure is typically completed in under an hour for most cases. Understand the risks associated with this procedure and how proper planning and sterile technique ensure safe, predictable results with minimal discomfort.
Integration with the Jawbone
Over time, your body gradually replaces the graft material with your own natural bone. This process is called osseointegration. It usually takes a few months, though the exact timeline depends on the graft size and your overall bone health. During this period, blood vessels grow into the graft and new bone cells form around it. This creates a strong, living foundation ready to support a dental implant securely.
Types of Bone Graft Materials
Understanding your options helps you make informed choices.
Autograft (Your Own Bone)
Harvested from another area of your body, such as your hip or chin, an autograft offers the best possible compatibility. This is because it comes from your own living tissue. It requires two surgical sites, which means a slightly longer recovery, but it integrates exceptionally well with no rejection risk. Autograft bone is widely considered the best material for dental implants when bone quality and stability are the priority.
Allograft (Donor Bone)
Sourced from a human donor, allografts are thoroughly processed, sterilized, and screened to ensure they're completely safe for use. This option avoids the need for an extra surgical site. That means less discomfort and a faster overall recovery for the patient. Allografts are a popular choice for patients who want reliable bone regeneration without the added healing time of harvesting their own bone tissue.
Xenograft (Animal Source)
Typically sourced from bovine (cow) bone, xenografts are well-processed, purified, and commonly used in dental restoration worldwide. They act as a scaffold that slowly resorbs as your own bone grows in to replace it over several months. Explore the Top dental implants in Turkey and why patients choose these reliable graft materials for long-lasting, stable smiles built on a solid foundation.
Synthetic Materials (Alloplast)
Made from minerals like calcium phosphate, synthetic materials are excellent for patients seeking non-biological graft options. There's no donor or animal tissue involved. These materials are manufactured under strict quality controls, offering consistent, predictable results with minimal infection risk. Synthetic grafts are especially popular for smaller defects or ridge preservation cases, where a fully synthetic scaffold is enough to support healthy new bone growth.
Dental Bone Graft Healing Stages
Healing after a dental bone graft happens in stages, moving from initial swelling and tenderness in the first days, to soft tissue closure over the following weeks, and finally full bone integration over several months. Each stage builds on the last, so rushing recovery or skipping follow-ups can slow the process down. At Vitrin Clinic, your healing is monitored closely at every stage to confirm you're progressing safely toward implant placement.
What to Expect Immediately After Surgery
You may experience swelling, mild pain, and limited mouth movement in the first few days after surgery. Ice packs and prescribed medication help manage these symptoms effectively during this initial period. Most patients return to normal daily activities within a few days. Strenuous exercise and hard foods should be avoided, though, until your Vitrin Clinic dentist confirms the surgical site is stable and healing well.
Recovery Timeline Week by Week
Week 1-2: Swelling subsides, stitches may be removed
Week 3-4: Soft tissue heals
Months 3-6: Bone integrates and strengthens
Check the Dental implants cost in Turkey to plan your investment in a beautiful smile. Also learn When to get an implant after this procedure for optimal healing and success. Following this week-by-week timeline closely, alongside your dentist's instructions, gives you the best chance of a smooth recovery. Most patients notice steady improvement at every stage, with little discomfort by the final months.
When Can You Get Your Dental Implant?
Most patients are ready for tooth implants 4–6 months after this treatment, depending on healing progress and graft complexity. Simpler grafts may allow for earlier implant placement. Larger reconstructions, such as block grafts, typically require additional healing time. Your Vitrin Clinic implantologist confirms readiness through follow-up imaging. This ensures the graft has fully integrated and can safely support your new implant long-term.
Benefits and Risks of Dental Bone Grafting
Like any surgical procedure, bone grafting comes with both clear benefits and some manageable risks worth understanding beforehand. The benefits include restored bone volume, stronger implant stability, and a healthier facial structure long-term. The risks, such as infection or mild swelling, are uncommon and easily managed with proper aftercare. At Vitrin Clinic, careful planning and experienced hands keep the benefits high and the risks as low as possible.
Key Benefits for Long-Term Implant Success
Bone grafting restores lost bone volume, giving your jaw the density needed to support a dental implant securely for years to come. It also improves implant stability, reducing the risk of failure or shifting after placement. Beyond function, it also prevents facial sagging caused by long-term bone loss. This helps preserve a natural, youthful facial structure and supports overall oral health well into the future.
Common Risks and Complications
As with any surgical procedure, this treatment carries some risks, though serious complications are uncommon when performed by experienced specialists. Infection is the most frequently reported issue, usually manageable with antibiotics and proper aftercare. Graft rejection is rare, particularly with biocompatible materials like allografts or synthetics. Mild swelling or discomfort is normal and temporary, usually fading within a week. Choosing an experienced clinic, like Vitrin Clinic, significantly reduces these risks through careful planning and close monitoring.
How to Reduce Healing Time and Avoid Infection
Following post-op instructions carefully is the single most important factor in fast, complication-free healing. Avoid smoking and alcohol, both of which slow blood flow and delay tissue repair. Keep the surgical area clean using any prescribed rinses. Avoid disturbing the site with your tongue or fingers. Attend all follow-up visits at Vitrin Clinic so any issues are caught and treated early.
How Much Does a Dental Bone Graft Cost?
The cost of a dental bone graft varies widely depending on the material used, the size of the graft, and whether the procedure is simple or complex. Prices generally range from $300 for minor grafts to $3,000 or more for advanced cases like sinus lifts. Vitrin Clinic offers transparent pricing and flexible payment plans well below USA, UK, and Europe rates. Every consultation is provided completely free of charge.
Factors That Influence the Price
Several factors shape the final price of this procedure, so costs can vary noticeably between patients. The type of graft material used, whether autograft, allograft, xenograft, or synthetic, affects pricing directly. The size and location of the graft also matter. Larger or harder-to-reach areas require more material and time. Finally, whether it's a simple graft or a complex procedure, like a sinus lift, plays a major role.
Cost Breakdown: Simple vs Complex Grafts
Simple grafts typically cost between $300 and $800, covering minor ridge preservation or small-area grafting cases. Complex grafts or sinus lifts range from $1,000 to $3,000 or more. This reflects the added materials, time, and expertise required. Read about grafting procedures explained to understand the techniques and benefits. Explore the Mini dental implants guide for limited bone cases. Vitrin Clinic offers transparent pricing and flexible payment plans, plus your consultation is always free.
Is a Bone Graft Right for You?
A bone graft is right for you if imaging shows your jawbone is too thin, soft, or resorbed to safely anchor a dental implant on its own. It's also worth considering if you've had missing teeth for years, lost bone to infection or trauma, or want the strongest possible foundation for your implant. The only way to know for certain is a 3D scan and evaluation, which Vitrin Clinic provides free of charge.
Tips for Patients
A little preparation goes a long way toward a smooth recovery. Eat soft foods like soup, yogurt, and mashed vegetables for the first few days, and steer clear of anything hard, crunchy, or chewy that could disturb the surgical site. Sleep with your head slightly elevated to reduce swelling, and use a cold compress on the outside of your cheek during the first 48 hours. Skip smoking, alcohol, and vigorous exercise until your Vitrin Clinic dentist gives you the go-ahead, since all three slow blood flow and delay healing. Rinse gently with any prescribed solution rather than brushing directly over the area, and never skip a follow-up appointment, even if you feel completely fine. Small habits like these are often what separate a fast, uneventful recovery from a longer one.
Who Is a Good Candidate for Bone Grafting?
You may be a good candidate if:
You have insufficient jawbone for implants
You're in good general health
You're committed to long-term oral health
At Vitrin Clinic, our experienced implantologists will evaluate your needs and provide a personalized treatment plan, starting with a free consultation. Even patients with significant bone loss are usually good candidates once the right grafting technique, healing time, and follow-up care are planned properly. This gives nearly everyone a realistic path toward a stable, long-lasting dental implant and a fully restored, confident smile.
Advanced Bone Grafting Techniques in Implantology
Beyond standard grafting, Vitrin Clinic offers advanced grafting techniques for patients with more complex bone loss patterns. These specialized methods allow our implantologists to rebuild the jaw with precision. This applies even in cases where a simple graft isn't enough to support a dental implant safely. From socket preservation to full sinus lifts, each technique is chosen based on your bone density, defect size, and long-term implant goals.
Alveolar Ridge Preservation (Socket Grafting)
Alveolar ridge preservation, or socket grafting, is performed immediately after a tooth extraction to stop the natural collapse of the jawbone. By placing graft material directly into the empty socket, we preserve the width and height of the ridge before major shrinkage occurs. This makes future implant placement significantly easier and more predictable. It's often recommended for patients planning a dental implant later in their treatment journey.
Sinus Lift Procedures for Upper Jaw Alignment
A sinus lift raises the sinus floor to create more bone volume in the upper back jaw, an area where bone is naturally thinner. This procedure is essential when the sinus sits too close to the jaw for an implant to be placed safely. At Vitrin Clinic, sinus lifts are planned using detailed 3D imaging. This ensures precise, comfortable, and predictable results for every patient.
Guided Bone Regeneration (GBR) and Bone Membranes
Guided bone regeneration uses a protective membrane to protect the grafted area while new bone forms underneath it. The membrane acts as a barrier, keeping soft tissue from growing into the graft site too quickly. This technique is one of the most reliable ways to rebuild bone volume before or during implant placement. It works especially well for moderate ridge defects and localized bone loss.
Block Bone Grafts for Severe Bone Loss
Block bone grafts are used when patients have significant bone loss that smaller grafting techniques can't correct on their own. A solid block of bone, often harvested from the patient's own jaw or hip, is secured in place with tiny screws. This rebuilds the deficient area. This technique requires a longer healing period, but it offers an exceptionally strong foundation for future implant placement.
Horizontal vs. Vertical Bone Regeneration
Horizontal bone regeneration widens a jawbone that has become too thin from side to side to support an implant securely. Vertical bone regeneration, by contrast, adds height to bone that has resorbed downward over time, often after long-term tooth loss. Choosing between them depends on your specific bone loss pattern, identified through detailed 3D imaging. Vitrin Clinic's team tailors the regeneration approach to each patient's unique anatomy.
Clinical Note
Dr. Rifat Alsaman, Head of the Medical Team and cosmetic dentist at Vitrin Clinic, notes that timing and imaging accuracy matter more than the material chosen in most cases. He points out that patients who follow the recommended healing window before implant placement, rather than rushing ahead, see meaningfully better long-term integration. He also flags that mild, temporary swelling is normal and not a sign of failure, but persistent pain, fever, or discharge after the first week always warrants a same-week check-up rather than a wait-and-see approach.
Pre-Surgical Protocols: Preparing for a Dental Bone Graft
Preparing for a dental bone graft surgery starts with a full medical and dental evaluation, including 3D imaging to map your bone density and jaw structure precisely. Patients are usually asked to avoid smoking, blood thinners, and alcohol in the days before surgery. This reduces bleeding and supports healing. At Vitrin Clinic, this preparation phase is guided step-by-step, so patients arrive fully informed, relaxed, and comfortable on surgery day.
Clinical Alternatives to Jaw Bone Grafting Surgery
Not every patient needs this procedure before getting a dental implant. Alternatives to this treatment include short or narrow-diameter implants that fit smaller bone areas without additional augmentation. All-on-4 techniques anchor implants in the jaw's denser regions, and zygomatic implants suit patients with severe upper jaw bone loss. Your Vitrin Clinic implantologist will assess your bone volume to determine whether an alternative can safely avoid grafting.
Medical Legalities: Giving Your Official Informed Consent (Permission)
Before any bone graft or implant procedure, Vitrin Clinic requires official informed consent from every patient without exception. This means you'll receive a full explanation of the procedure, materials used, expected outcomes, and possible risks in your own language. You'll also have plenty of time to ask questions. Signing this consent confirms you fully understand and agree to the treatment plan. It protects both your rights as a patient and the transparency of your care.
What We Notice Clinically
Dr. Rifat Alsaman, Head of the Medical Team and cosmetic dentist at Vitrin Clinic, notes that patients who undergo guided bone regeneration or socket grafting right after extraction tend to need less extensive grafting later. This is because the ridge is preserved before major bone loss occurs. He also observes that block grafts, though requiring longer healing, consistently give patients the stable foundation needed for long-term implant success. He stresses that careful planning and clear informed consent prevent most complications.
About Vitrin Clinic
Vitrin Clinic is a cosmetic dental clinic in Istanbul, Turkey, trusted by international patients seeking advanced, affordable dental care. Our team combines modern technology, including 3D imaging and guided bone regeneration, with a patient-first approach to every grafting and implant case. Led by Dr. Rifat Alsaman, Head of the Medical Team and cosmetic dentist at Vitrin Clinic, our specialists guide patients through every step. That means from free consultation to full recovery and a confident smile.
Ready to Restore Your Smile with Vitrin Clinic?
If you're exploring this procedure for a dental implant, contact Vitrin Clinic today to schedule your free consultation. Take the first step toward a healthier, more confident smile. Discover the Types of grafts for dentistry and how each type supports implant success. Learn about Recovery after this surgery and tips for a smooth, safe healing process from start to finish.
References:
FAQs

Dr. Rifat Alsaman has more than 5 years of clinical experience in dentistry and currently serves as the Head of the Medical Team at Vitrin Clinic. He is dedicated to providing exceptional patient care, overseeing treatment planning, and ensuring the highest clinical standards across the team. His expertise, attention to detail, and commitment to continuous professional development have helped countless patients achieve healthier, more confident smiles.

.webp&w=3840&q=75)



